Associate Clinical Educators™ vs. Simulated Patients: Defining Roles in Medical Education
Associate Clinical Educators™ vs. Simulated Patients: Defining Roles in Medical Education In the...
Read More
Associate Clinical Educators™ vs. Simulated Patients: Defining Roles in Medical Education In the...
Read More
In medical education, the term “patient journey” refers to the comprehensive pathway a...
Read MoreIn this article, we explore the role of ACEs in healthcare education and the importance of effective communication skills. We discuss the impact of active listening on building rapport with patients and avoiding...
Read MoreIf you’re an Associate Clinical Educator (ACE), you may have wondered what sets you apart from a simulated patient or medical role player. In this article, we will be exploring this question and providing a useful...
Read MoreThe Bootcamp for Physician Associate students at Chester University is an intensive training program designed to help students prepare for National Exams. It involves practising skills, receiving feedback from experienced...
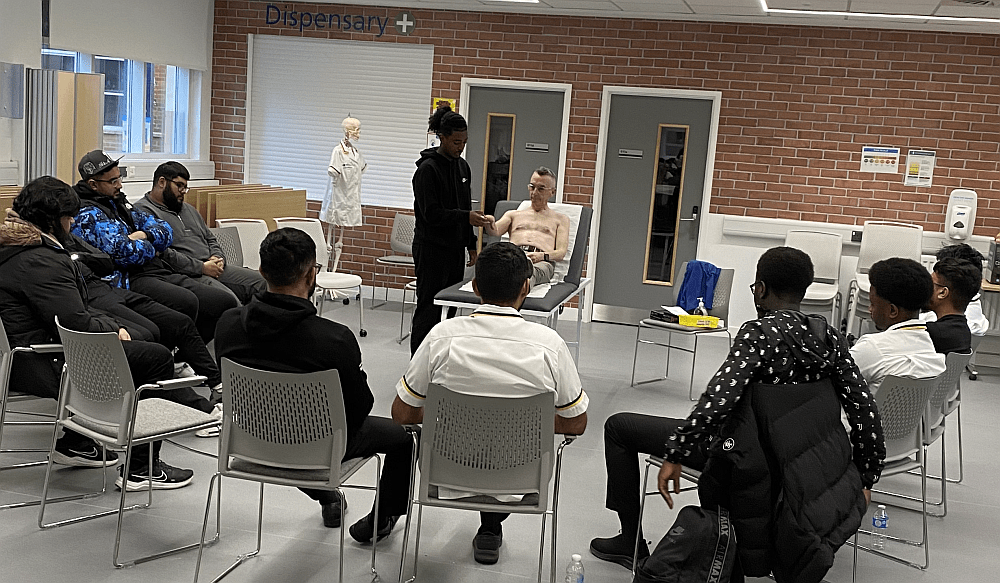
Read MoreMeducate Academy were recently invited down to The Drummond Education Centre West Suffolk Hospital to demonstrate the role of the ACE to a group of 1st and 2nd year Physician Associates. The vast majority of the day was spent...
Read MoreThe past month has been frantic! Both of our partners (Wolverhampton and Chester University) have kept us busy with both their 1st and 2nd year cohorts. We have sent teams of ACEs out, providing hi-fidelity teaching and...
Read MoreRecently my attention was drawn to an article, ‘It’s Not An Acting Job … Don’t Underestimate What A Simulated Patient Does”: A Qualitative Study Exploring the Perspectives of Simulated Patients in Health...
Read MoreJames Ennis is currently Clinical Lead at The University of Chester Physician Associate Programme. He has worked with ACEs both as student Physician Associate, and also used ACEs when he was teaching at The University of...
Read MoreProfessor Parle was our keynote speaker at the conference and it was an honour to have him join us. What follows is an abridged version of the talk. If you want to view the complete talk it is available in the video above....
Read MoreIt’s always important for an ACE to understand the protocols health professionals must follow to help them take a good history from a patient. Once we understand this we are able to give hi-fidelity feedback to the...
Read More