A Note of Thanks From Meducate Academy — A Moment of Reflection
A Note of Thanks From Meducate Academy — A Moment of Reflection As the year draws to a close, it...
Read More

A Note of Thanks From Meducate Academy — A Moment of Reflection As the year draws to a close, it...
Read More
Empowering Ethical Learning Through Strategic Collaboration Introduction Modern medical education...
Read More
Intro Pharmacists are among the most accessible healthcare professionals, often serving as the...
Read More
In today’s fast-paced and ever-evolving healthcare landscape, doctors, nurses, and medical professionals embark on journeys that mirror the classic hero’s path—filled with trials, transformation, and triumph. This article explores The Hero’s Journey through the lens of modern healthcare, revealing how those in medicine face emotional and physical challenges, grow through mentorship, and return with hard-earned wisdom to heal others. By blending mythology, storytelling, and real-life medical experiences, we highlight the profound personal and professional evolution that defines a career in healthcare.
Read More
Medicine has always carried an expectation of certainty. Patients seek definitive answers....
Read More
Struggling with your OSCEs? Want to ensure a spectacular failure? The Objective...
Read More
Meducate Academy is at the forefront of pharmacy education, equipping pharmacists with the skills...
Read More
Critical Thinking and Writing for Undergraduate Pharmacists Developing critical thinking and...
Read More
Physician Associates (PAs) are becoming indispensable in modern healthcare, bridging gaps in...
Read More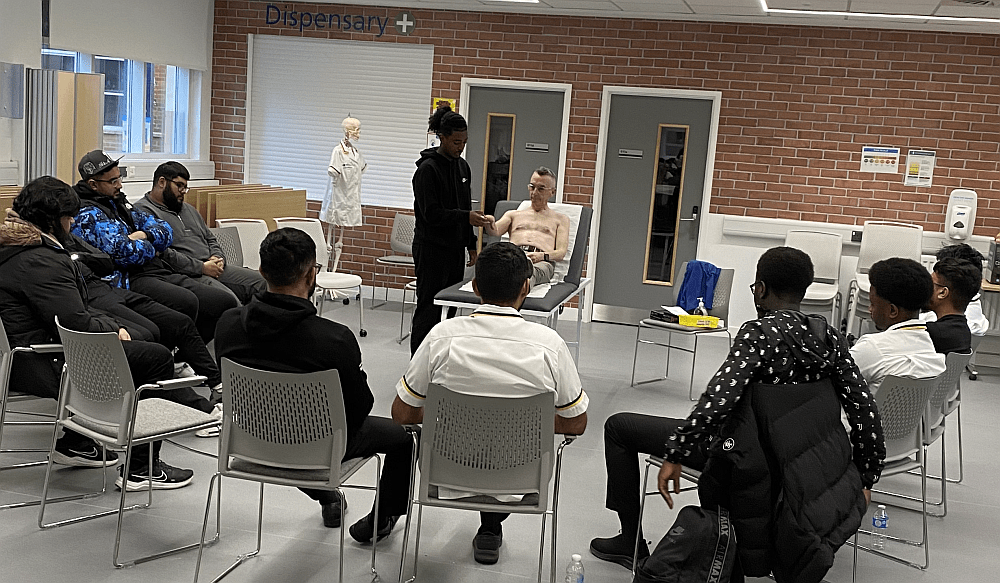
Associate Clinical Educators™ vs. Simulated Patients: Defining Roles in Medical Education In the...
Read More
Boost Your Clinical Skills: Join the Pharmacist Workshop in Birmingham in March 2025! After a...
Read More Welcome to Meducate Academy’s 2nd year running Interactive Workshops at The Pharmacy Show...
Read More